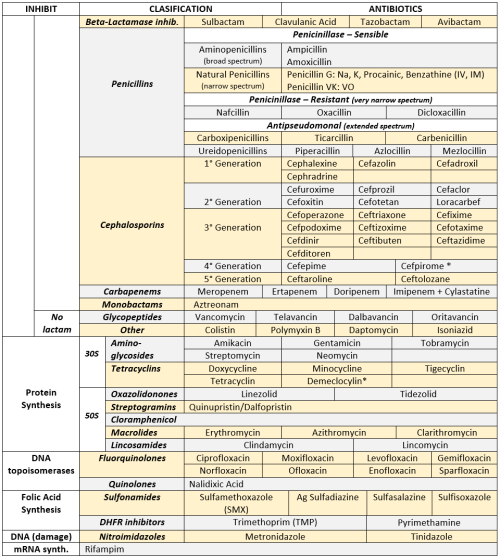
ANTIBIOTICS CHEAT SHEET :)
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci

* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines

* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones
More Posts from Fuadalanazi and Others
الشيخ عبد الباسط عبد الصمد(التكوير و سورة القدر)روعة (by theeslamcena)









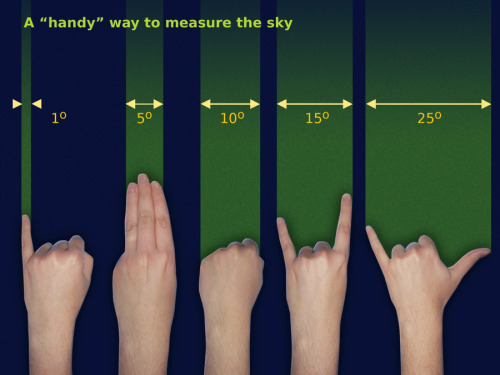
Measuring the sky, the handy way.
Source: Free Astronomy Teaching Resources (Starry Night)
A Basic Demonstration of Optical Cloaking (by UniversityRochester)
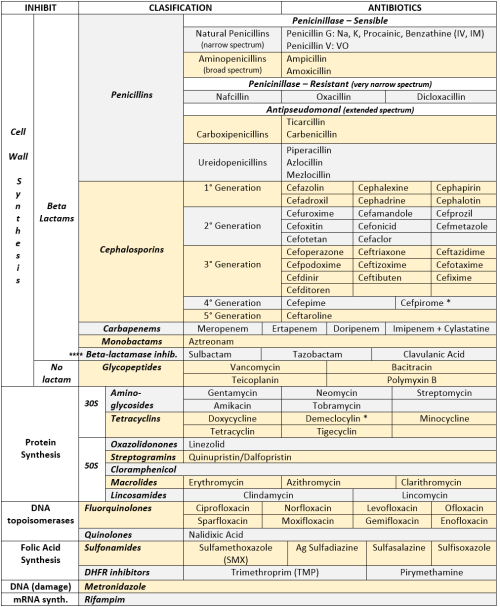
ANTIBIOTICS CHEAT SHEET :)
Also, REMEMBER!!!!
* Sulfonamides compete for albumin with:
Bilirrubin: given in 2°,3°T, high risk or indirect hyperBb and kernicterus in premies
Warfarin: increases toxicity: bleeding
* Beta-lactamase (penicinillase) Suceptible:
Natural Penicillins (G, V, F, K)
Aminopenicillins (Amoxicillin, Ampicillin)
Antipseudomonal Penicillins (Ticarcillin, Piperacillin)
* Beta-lactamase (penicinillase) Resistant:
Oxacillin, Nafcillin, Dicloxacillin
3°G, 4°G Cephalosporins
Carbapenems
Monobactams
Beta-lactamase inhibitors
* Penicillins enhanced with:
Clavulanic acid & Sulbactam (both are suicide inhibitors, they inhibit beta-lactamase)
Aminoglycosides (against enterococcus and psedomonas)
* Aminoglycosides enhanced with Aztreonam
* Penicillins: renal clearance EXCEPT Oxacillin & Nafcillin (bile)
* Cephalosporines: renal clearance EXCEPT Cefoperazone & Cefrtriaxone (bile)
* Both inhibited by Probenecid during tubular secretion.
* 2°G Cephalosporines: none cross BBB except Cefuroxime
* 3°G Cephalosporines: all cross BBB except Cefoperazone bc is highly highly lipid soluble, so is protein bound in plasma, therefore it doesn’t cross BBB.
* Cephalosporines are "LAME“ bc they do not cover this organisms
L isteria monocytogenes
A typicals (Mycoplasma, Chlamydia)
M RSA (except Ceftaroline, 5°G)
E nterococci
* Disulfiram-like effect: Cefotetan & Cefoperazone (mnemonic)
* Cefoperanzone: all the exceptions!!!
All 3°G cephalosporins cross the BBB except Cefoperazone.
All cephalosporins are renal cleared, except Cefoperazone.
Disulfiram-like effect
* Against Pseudomonas:
3°G Cef taz idime (taz taz taz taz)
4°G Cefepime, Cefpirome (not available in the USA)
Antipseudomonal penicillins
Aminoglycosides (synergy with beta-lactams)
Aztreonam (pseudomonal sepsis)
* Covers MRSA: Ceftaroline (rhymes w/ Caroline, Caroline the 5°G Ceph), Vancomycin, Daptomycin, Linezolid, Tigecycline.
* Covers VRSA: Linezolid, Dalfopristin/Quinupristin
* Aminoglycosides: decrease release of ACh in synapse and act as a Neuromuscular blocker, this is why it enhances effects of muscle relaxants.
* DEMECLOCYCLINE: tetracycline that’s not used as an AB, it is used as tx of SIADH to cause Nephrogenic Diabetes Insipidus (inhibits the V2 receptor in collecting ducts)
* Phototoxicity: Q ue S T ion?
Q uinolones
Sulfonamides
T etracyclines
* p450 inhibitors: Cloramphenicol, Macrolides (except Azithromycin), Sulfonamides
* Macrolides SE: Motilin stimulation, QT prolongation, reversible deafness, eosinophilia, cholestatic hepatitis
* Bactericidal: beta-lactams (penicillins, cephalosporins, monobactams, carbapenems), aminoglycosides, fluorquinolones, metronidazole.
* Baceriostatic: tetracyclins, streptogramins, chloramphenicol, lincosamides, oxazolidonones, macrolides, sulfonamides, DHFR inhibitors.
* Pseudomembranous colitis: Ampicillin, Amoxicillin, Clindamycin, Lincomycin.
* QT prolongation: macrolides, sometimes fluoroquinolones
(via https://www.youtube.com/watch?v=eP085YW60D8)

No bacterium is an island.
Many people think of bacteria as tiny Lone Rangers, paddling their flagellar canoes across the desolate petri dish sea. But in “the wild”, bacteria exist as complex, interwoven, constantly competing social communities.
Every scoop of soil is a battlefield of chemical chatter. Species send out molecular messages-in-a-bottle that ride the waves of diffusion to their mates. Some even thread electrical cables between neighboring cells. Now, new research has identified elaborate shared membranes that let single cells swarm as a superorganism …
Check out my latest article for Wired all about a soil bacterium named Myxococcus xanthus. It’s under everyone’s feet right now, and it has developed one of the most elaborate physical webs ever witnessed in bacteria. That’s it up top, devouring a colony of E. coli using its patented rippling wave attack.
It’s a stealth communication network that lets them hunt like a tiny wolfpack. So cool. Plus I got to use a GIF, so double win.
Once you’re done with that, check out this great TED talk from Bonnie Bassler all about how bacteria communicate.

“Sequence VR" was exhibited at the V & A Museum in London, as part of the London Design Festival. A new immersive virtual reality experience has been created using an Oculus Rift as part of “Sequence” using the data and footage from the project. It was shown alongside a series of objects and artefacts created during the project including live bacteria. The exhibit was accompanied by a participatory DNA extraction/preparation workshop where Dumitriu was joined by Dr Nicola Fawcett from the Modernisng Medical Microbiology Project. The event took place on 25th - 27th September 2015. See more information here.
-
 2025bs2026 liked this · 1 month ago
2025bs2026 liked this · 1 month ago -
 ant-heia liked this · 2 months ago
ant-heia liked this · 2 months ago -
 tooearthquakekoala liked this · 5 months ago
tooearthquakekoala liked this · 5 months ago -
 tmarkmulles liked this · 6 months ago
tmarkmulles liked this · 6 months ago -
 sunfortune liked this · 8 months ago
sunfortune liked this · 8 months ago -
 crimsonrebel liked this · 8 months ago
crimsonrebel liked this · 8 months ago -
 muwanguzi-01 liked this · 9 months ago
muwanguzi-01 liked this · 9 months ago -
 okbro-wegetit liked this · 9 months ago
okbro-wegetit liked this · 9 months ago -
 adennnsstuff liked this · 10 months ago
adennnsstuff liked this · 10 months ago -
 daddysbunnypixie liked this · 11 months ago
daddysbunnypixie liked this · 11 months ago -
 allecrax liked this · 1 year ago
allecrax liked this · 1 year ago -
 micazin liked this · 1 year ago
micazin liked this · 1 year ago -
 jingerlei liked this · 1 year ago
jingerlei liked this · 1 year ago -
 perla-estrada-universe liked this · 1 year ago
perla-estrada-universe liked this · 1 year ago -
quantumdoctor15 liked this · 1 year ago
-
 cerebrology reblogged this · 1 year ago
cerebrology reblogged this · 1 year ago -
 hopenada reblogged this · 1 year ago
hopenada reblogged this · 1 year ago -
hopenada liked this · 1 year ago
-
 semie78 liked this · 1 year ago
semie78 liked this · 1 year ago -
 ngugikamau liked this · 1 year ago
ngugikamau liked this · 1 year ago -
 atomicstarburstlabware reblogged this · 1 year ago
atomicstarburstlabware reblogged this · 1 year ago -
 yahajbaba liked this · 1 year ago
yahajbaba liked this · 1 year ago -
 louis7473 liked this · 1 year ago
louis7473 liked this · 1 year ago -
 hellohiomg-blog reblogged this · 1 year ago
hellohiomg-blog reblogged this · 1 year ago -
hellohiomg-blog liked this · 1 year ago
-
 basicallyarganine liked this · 1 year ago
basicallyarganine liked this · 1 year ago -
 provokinq liked this · 1 year ago
provokinq liked this · 1 year ago -
 pabsitiltogis liked this · 1 year ago
pabsitiltogis liked this · 1 year ago -
 conkecounpimpflow liked this · 1 year ago
conkecounpimpflow liked this · 1 year ago -
 wtrsine88 liked this · 1 year ago
wtrsine88 liked this · 1 year ago -
 ticserupma liked this · 1 year ago
ticserupma liked this · 1 year ago -
 maincarescha liked this · 1 year ago
maincarescha liked this · 1 year ago -
 styllenhardwen liked this · 1 year ago
styllenhardwen liked this · 1 year ago -
 gonsuheci liked this · 1 year ago
gonsuheci liked this · 1 year ago -
 webedragons liked this · 1 year ago
webedragons liked this · 1 year ago -
 studyhard2studyabroad reblogged this · 1 year ago
studyhard2studyabroad reblogged this · 1 year ago -
 kuromegami liked this · 1 year ago
kuromegami liked this · 1 year ago